
[accordion_item title=”CASE 1 -37 year old woman, with type I DM, hypothyroidism, presenting with poor appetite, weight loss, epigastric pain and frequent hypoglycemia. “]
37 year old woman with type I DM and hypothyroidism, well controlled, presents for follow-up. She complains of poor appetite, 10 lbs weight loss over 3 months, mild intermittent epigastric pain. ROS otherwise negative. Exam is unremarkable. HbA1C = 7.2%, no recent changes to insulin regimen. Review of BGs shows frequent hypoglycemia, otherwise normal range BGs. Labs shows normal CBC, BMP with Na of 129, K 5.2, Cr & BUN normal; hepatic panel nl, TSH & free T4 normal.
What lab do you order to confirm your suspected diagnosis?

What is the (specific) diagnosis? Extra: how might you manage this patient?
What medication(s), dosages and timing would you use for medical management of her miscarriage?
Vitals are: afebrile, HR 110, BP 130/80, RR 18, SaO2 100% on ambient air. He is in no acute distress. + conjunctival pallor. Abdominal exam is benign. Rectal exam shows no blood. Skin exam is notable for the rash below. Laboratory tests showing an Hct of 18%, MCV 62, ferritin 5 ng/mL, transferrin iron saturation of 4%, 25-hydroxy-vitamin D of 11 ng/mL.

In addition to inflammatory bowel disease, what one other diagnosis is high on the differential?
Prior testing showed him to be HIV and HCV seronegative, HBV immune. Repeat assays today show HIV antigen/antibody screening assay to be positive, HIV Western blot negative, and HIV PCR positive – all consistent with acute retroviral syndrome. Further laboratory work-up is done, showing a CD4 count of 654 cells/microL and an HIV viral load of 84,650 copies/mL. Other routine tests are performed and return within normal limits. He returns one week later, citing readiness to start antiretroviral therapy.
At what point would you recommend that he start HIV treatment with antiretroviral therapy? Bonus: what is one recommended first-line regimen in the United States?
Pharmacotherapy with what other agent would likely reduce the mortality risk in this patient?
Does this patient require treatment with antivirals? Does this patient require an ultrasound for hepatocellular carcinoma screening?
In her case, what is her risk class according to the Revised Cardiac Risk Index for pre-operative risk? And according to the American College of Surgeons Surgical Risk Calculator?
Given the duration and worsening pain, radiographs were obtained, with area of interested highlighted here:

What is the likely diagnosis? What are your next steps in work-up or management?
What would be your recommendations to reduce this gentleman’s risk of developing future kidney stones?
When would you recommend starting screening mammograms? At what interval would you recommend they continue?
Bonus: For 1000 women at age 50, undergoing annual mammography for 10 years, how many deaths due to breast cancer would you estimate would be prevented? How many would be estimated to be overdiagnosed and treated, unnecessarily, with surgery, radiation or chemotherapy?
[/accordion_item]
[accordion_item title=”CASE 12 – 40 year old woman inquiring about mammography”]
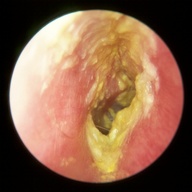
A 56 year old with history of HTN and type II diabetes controlled on oral hypoglycemics presents for left ear pain and pruritis. Symptoms began rapidly 7 days prior, reaching the current level of intensity within 24 hours after onset. Symptoms have persisted. He tried cleaning his left ear with a cotton q-tip, without any change in symptoms. He denies hear loss, tinnitus, fevers, chills, jaw pain. He has noted a minimal white-yellow discharge on his pillow. On exam, he is afebrile, normal vitals.
If he had little pain to tugging on the tragus and pinna, with an otoscopic exam as below, what might be your management?

If he had more significant pain and an otoscopic exam as below, what might be your management?
[/accordion_item]
What lab do you order to confirm your suspected diagnosis?
Answer
[/accordion_item]
[accordion_item title=”CASE 2 – 9 year old girl s/p fall”]
A 9 year old girl with no past medical history presents with left leg pain. She was playing earlier, jumped off of a 7 foot fence, landing on her feet prior to onset of pain. There was no head, pelvic or abdominal injury. Her vitals are notable for sinus tachycardia. She is grimacing, refusing to ambulate. Exam shows pain superior to the medial malleolus with minor ecchymoses and significant localized edema. A radiograph taken:
AM serum cortisol stimulation test
Discussion:
Her symptoms of anorexia (poor appetite), weight loss, abdominal pain are suggestive of adrenal insufficiency, amongst other possible causes. Due to a decrease in serum cortisol levels in adrenal insufficiency, patients with diabetes will note a reduce insulin requirement; or rather, by using the same insulin regimen, patients may note more frequent episodes of hypoglycemia. Dangerously, asymptomatic hypoglycemia is more common in adrenal insufficiency (for those using insulin). Her mild hyponatremia and hyperkalemia are consistent with adrenal insufficiency.
Patients with autoimmune endocrinopathies (eg type I diabetes, hypothyroidism secondary to Hashimoto’s thyroiditis) are at higher risk of other autoimmune endocrinopathies (eg autoimmune adrenalitis, autoimmune hypoparathyroidism). The triad of type I diabetes, autoimmune hypothyroidism and autoimmune adrenalitis forms the autoimmune polyendocrinopathy syndrome type II.
When adrenal insufficiency is suspected, start with an AM (typically 8 am) serum cortisol stimulation test: Measure the serum cortisol level at 8 am, administer 250 mcg cosyntropin (synthetic ACTH), then measure serum cortisol 1 hour later. If there is an insufficient increase in serum cortisol, adrenal insufficiency is diagnosed. Then measure serum endogenous ACTH to determine if the disorder if primary (eg autoimmune adrenalitis) vs secondary (eg pituitary or hypothalamic disorder).
Further reading: Bornstein, N Engl J Med 2009; 360 : 2328
Discussion:
Her symptoms of anorexia (poor appetite), weight loss, abdominal pain are suggestive of adrenal insufficiency, amongst other possible causes. Due to a decrease in serum cortisol levels in adrenal insufficiency, patients with diabetes will note a reduce insulin requirement; or rather, by using the same insulin regimen, patients may note more frequent episodes of hypoglycemia. Dangerously, asymptomatic hypoglycemia is more common in adrenal insufficiency (for those using insulin). Her mild hyponatremia and hyperkalemia are consistent with adrenal insufficiency.
Patients with autoimmune endocrinopathies (eg type I diabetes, hypothyroidism secondary to Hashimoto’s thyroiditis) are at higher risk of other autoimmune endocrinopathies (eg autoimmune adrenalitis, autoimmune hypoparathyroidism). The triad of type I diabetes, autoimmune hypothyroidism and autoimmune adrenalitis forms the autoimmune polyendocrinopathy syndrome type II.
When adrenal insufficiency is suspected, start with an AM (typically 8 am) serum cortisol stimulation test: Measure the serum cortisol level at 8 am, administer 250 mcg cosyntropin (synthetic ACTH), then measure serum cortisol 1 hour later. If there is an insufficient increase in serum cortisol, adrenal insufficiency is diagnosed. Then measure serum endogenous ACTH to determine if the disorder if primary (eg autoimmune adrenalitis) vs secondary (eg pituitary or hypothalamic disorder).
Further reading: Bornstein, N Engl J Med 2009; 360 : 2328

What is the (specific) diagnosis? Extra: how might you manage this patient?
Answer
[/accordion_item]
[accordion_item title=”CASE 3 – 24 year old G1 at 8-1/7 with vaginal bleeding”]
An 24 year old G1 at 8-1/7 weeks gestation by LMP and a 7-week ultrasound presents for recent vaginal bleeding. She noted a small amount of bleeding and passage of clot & tissue earlier this morning. Bleeding has since ceased. She has no pain and is in no acute distress. She is afebrile with normal hemodynamics. Pelvic exam reveals minimal coagulated blood in the posterior vagina and a visible closed cervix. Bimanual exam shows an 6-7 week uterus and cervical exam of fingertip dilation. Transvaginal US reveals retained products of conception but no fetal heart tones. Hct is 39%, Rh factor is negative. She requests medical management of her incomplete abortion.
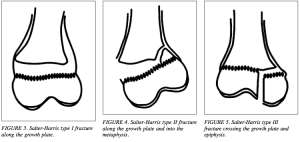
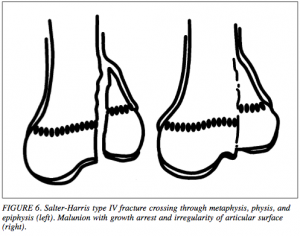
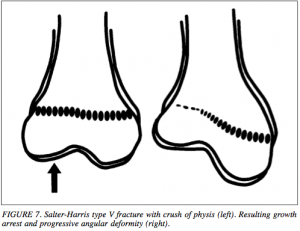
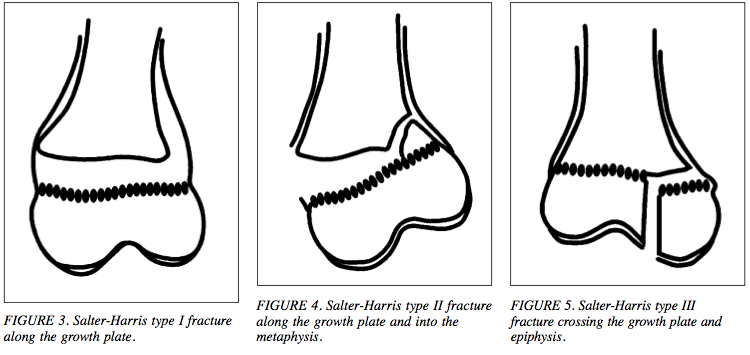
Salter-Harris type II fracture of the distal tibia
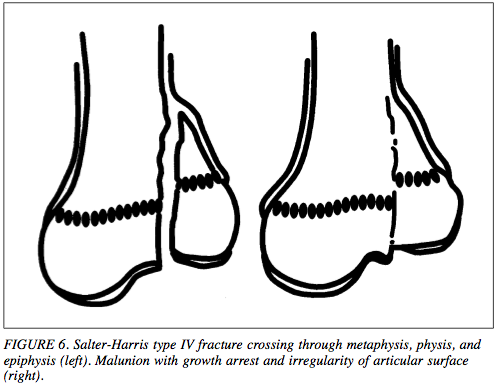
Discussion: This patient has a fracture extending from the metaphysis to the distal tibial physis (growth plate), but not into the epiphysis, categorized as a Salter-Harris type II fracture. Salter-Harris fractures are those that involve the physis (of any long bones). See the image below for a description of the 5 most commonly described SH fractures. This fracture, the SH type II fracture, is the most commonly seen fracture. It has an excellent prognosis and excellent remodeling capacity. Surgical intervention is often not necessary, as neither the epiphysis nor the articular (joint-space) cartilage are involved (involvement of either or both could lead to abnormal growth on the side of the bone with the fracture compared to the side without).
This patient would get another x-ray is the perpendicular plane to ensure to displacement; closed reduction if necessary; then casting (keeping in mind the potential for additional swelling). Follow-up in 1-2 weeks for repeat radiographs to ensure continued reduction and possible cast revision as swelling decreases. Casting & non-weight bearing x 4-6 weeks would be appropriate.
Discussion: This patient has a fracture extending from the metaphysis to the distal tibial physis (growth plate), but not into the epiphysis, categorized as a Salter-Harris type II fracture. Salter-Harris fractures are those that involve the physis (of any long bones). See the image below for a description of the 5 most commonly described SH fractures. This fracture, the SH type II fracture, is the most commonly seen fracture. It has an excellent prognosis and excellent remodeling capacity. Surgical intervention is often not necessary, as neither the epiphysis nor the articular (joint-space) cartilage are involved (involvement of either or both could lead to abnormal growth on the side of the bone with the fracture compared to the side without).
This patient would get another x-ray is the perpendicular plane to ensure to displacement; closed reduction if necessary; then casting (keeping in mind the potential for additional swelling). Follow-up in 1-2 weeks for repeat radiographs to ensure continued reduction and possible cast revision as swelling decreases. Casting & non-weight bearing x 4-6 weeks would be appropriate.

What medication(s), dosages and timing would you use for medical management of her miscarriage?
Answer
[/accordion_item]
[accordion_item title=”CASE 4 – 26 year old with fatigue & diarrhea”]
A 26 year old gentleman with no past medical history presents to clinic for fatigue and diarrhea. He notes increasing fatigue for the last 2 months, now associated with dyspnea on exertion and lightheadedness. He also notes diarrhea, often up to 5 times per day, for the last 12 months, sometimes with a small amount of blood mixed in. He denies any abdominal pain, fevers, or arthralgias. He has noted a 20 lbs unintentional weight loss over the last year.
Misoprostol 800 mcg vaginally (or could use buccally) once, followed by a 2nd dose if no response to the first; Rho(D) immune globulin 50 mcg IM once
Discussion:
This patient, with a previously confirmed intrauterine pregnancy, now presents with evidence of an incomplete spontaneous abortion (miscarriage): symptoms (bleeding) with no cardiac activity or fetal pole seen on transvaginal ultrasound (which would be expected at this gestational age). With a stable hematocrit and no signs/symptoms of infection, medical management is reasonable.
Misoprostol 800 mcg either vaginally (often recommended in this case) or buccally results in an estimated 70% efficacy rate for the 1st dose. If no bleeding after dose #1, a 2nd dose given 24-48 hours later improves overall efficacy rates to 84%. NSAIDs can be used for cramping. Anti-emetics for nausea. As she is Rh negative, Rho(D) immune globulin is indicated to prevent alloimmunization and potential problems in subsequent pregnancies with an Rh positive fetus. Follow-up by phone or in person 1-2 days after the first misoprostol, then 1 weeks in clinic to confirm completion of the miscarriage. Assess success by clinical history with either a 50% decline in quantitative beta-HCG or disappearance of IUP on transvaginal US, or a negative urine pregnancy test (which may take weeks to turn negative).
Counseling on the commonness of miscarriages and reassurance of the benign implications after 1 miscarriage is always a part of management.
Further reading: Nielson, Cochrane Database Syst Rev 2013; 3:CD007223.
Discussion:
This patient, with a previously confirmed intrauterine pregnancy, now presents with evidence of an incomplete spontaneous abortion (miscarriage): symptoms (bleeding) with no cardiac activity or fetal pole seen on transvaginal ultrasound (which would be expected at this gestational age). With a stable hematocrit and no signs/symptoms of infection, medical management is reasonable.
Misoprostol 800 mcg either vaginally (often recommended in this case) or buccally results in an estimated 70% efficacy rate for the 1st dose. If no bleeding after dose #1, a 2nd dose given 24-48 hours later improves overall efficacy rates to 84%. NSAIDs can be used for cramping. Anti-emetics for nausea. As she is Rh negative, Rho(D) immune globulin is indicated to prevent alloimmunization and potential problems in subsequent pregnancies with an Rh positive fetus. Follow-up by phone or in person 1-2 days after the first misoprostol, then 1 weeks in clinic to confirm completion of the miscarriage. Assess success by clinical history with either a 50% decline in quantitative beta-HCG or disappearance of IUP on transvaginal US, or a negative urine pregnancy test (which may take weeks to turn negative).
Counseling on the commonness of miscarriages and reassurance of the benign implications after 1 miscarriage is always a part of management.
Further reading: Nielson, Cochrane Database Syst Rev 2013; 3:CD007223.
Vitals are: afebrile, HR 110, BP 130/80, RR 18, SaO2 100% on ambient air. He is in no acute distress. + conjunctival pallor. Abdominal exam is benign. Rectal exam shows no blood. Skin exam is notable for the rash below. Laboratory tests showing an Hct of 18%, MCV 62, ferritin 5 ng/mL, transferrin iron saturation of 4%, 25-hydroxy-vitamin D of 11 ng/mL.

In addition to inflammatory bowel disease, what one other diagnosis is high on the differential?
Answer
[/accordion_item]
[accordion_item title=”CASE 5 – 42 year old with acute retroviral syndrome”]
A 42 year old gentleman with history of intravenous drug use presents to clinic. His opioid addiction had been in remission for 5 years; however, he relapsed once, three weeks prior. He has since reconnected with his methadone replacement therapy clinic and addictions counseling and reports no cravings for opiates. One week prior, he began experiencing daily atypical headaches, low-grade fever, malaise, myalgias and arthralgias. These have improved but are continuing.
Celiac disease
Discussion: Symptoms of chronic diarrhea are non-specific, but can be seen with celiac disease. The markedly low transferrin saturation and ferritin help explain the severe microcytic anemia (causing the fatigue and dyspnea on exertion), and together with vitamin D deficiency and weight loss, suggest a malabsorption syndrome. IBD & celiac would be two diagnoses high on the differential. Other less likely possibilities would include pancreatic insufficiency (secondary to alcohol or cystic fibrosis), lactase deficiency, bacterial overgrowth (no risk factors in this young man), or a protein-losing gastroenteropathy. In celiac, as with IBD, transaminases would be expected to be elevated. The rash pictured is consistent with dermatitis herpetiformis, a blistering rash with pathognomonic IgA deposits – a rare sign of celiac. Celiac can often present “silently” – with only lab abnormalities found (eg anemia, vit D deficiency, transaminitis), without symptoms.
IgA anti-tissue transglutaminase antibodies have the highest sensitivity and specificity and are recommended as a first-line screening test (also get a total IgA to ensure no general IgA deficiency, which would affect the usability of the anti-ttG assay). Endoscopy with biopsies would offer definitive evidence.
Further reading: Fasano, NEJM 2012; 367:2419.
Discussion: Symptoms of chronic diarrhea are non-specific, but can be seen with celiac disease. The markedly low transferrin saturation and ferritin help explain the severe microcytic anemia (causing the fatigue and dyspnea on exertion), and together with vitamin D deficiency and weight loss, suggest a malabsorption syndrome. IBD & celiac would be two diagnoses high on the differential. Other less likely possibilities would include pancreatic insufficiency (secondary to alcohol or cystic fibrosis), lactase deficiency, bacterial overgrowth (no risk factors in this young man), or a protein-losing gastroenteropathy. In celiac, as with IBD, transaminases would be expected to be elevated. The rash pictured is consistent with dermatitis herpetiformis, a blistering rash with pathognomonic IgA deposits – a rare sign of celiac. Celiac can often present “silently” – with only lab abnormalities found (eg anemia, vit D deficiency, transaminitis), without symptoms.
IgA anti-tissue transglutaminase antibodies have the highest sensitivity and specificity and are recommended as a first-line screening test (also get a total IgA to ensure no general IgA deficiency, which would affect the usability of the anti-ttG assay). Endoscopy with biopsies would offer definitive evidence.
Further reading: Fasano, NEJM 2012; 367:2419.
Prior testing showed him to be HIV and HCV seronegative, HBV immune. Repeat assays today show HIV antigen/antibody screening assay to be positive, HIV Western blot negative, and HIV PCR positive – all consistent with acute retroviral syndrome. Further laboratory work-up is done, showing a CD4 count of 654 cells/microL and an HIV viral load of 84,650 copies/mL. Other routine tests are performed and return within normal limits. He returns one week later, citing readiness to start antiretroviral therapy.
At what point would you recommend that he start HIV treatment with antiretroviral therapy? Bonus: what is one recommended first-line regimen in the United States?
Answer
[/accordion_item]
[accordion_item title=”CASE 6 – 58 year old with heart failure”]
A 58 year old gentleman is seen in clinic for the management of heart failure with a reduced ejection fraction. The etiology of his heart failure is secondary to ischemic cardiomyopathy. He has symptoms of dyspnea with moderate exertion, otherwise he feels well. He takes aspirin, lisinopril, metoprolol succinate, furosemide, and atorvastatin. His blood pressure is 130/80, HR 76, SpO2 98% on ambient air. His last transthoracic echocardiogram 3 months ago showed a LVEF of 30%, stable compared to 1 year prior. Labs show Na 134, K 4.1, Cr 1.3, Hct 36%.
Start ART immediately, regardless of CD4 count, when the person is ready (exceptions may occur in the setting of certain opportunistic infections and for ‘elite controllers’)
Discussion:
Whereas prior guidelines recommended a CD4 count threshold below which HIV therapy should be initiated, newer evidence suggests both clinical benefit to the individual and significant gains in reduction of HIV transmission with initiation of therapy at CD4 counts above 500 cells/microL. Benefits to the individual include lower viral set point, better immune reconstitution after therapy is started, and high CD4 count increases. HIV transmission is reduced by an estimated 95% for those on therapy.
First-line treatment regimens include two nucleotide/nucleoside reverse transcriptase inhibitors (abacavir/lamivudine or tenofovir/emtracitabine) with either an integrase inhibitor (eg dolutegravir, elvitegravir, or raltegravir), a non-nucleoside reverse transcriptase inhibitor (eg efavirenz), or a ritonavir-boosted protease inhibitor (eg darunavir, atazanavir).
Further reading: JAMA 2014; 312:410
Discussion:
Whereas prior guidelines recommended a CD4 count threshold below which HIV therapy should be initiated, newer evidence suggests both clinical benefit to the individual and significant gains in reduction of HIV transmission with initiation of therapy at CD4 counts above 500 cells/microL. Benefits to the individual include lower viral set point, better immune reconstitution after therapy is started, and high CD4 count increases. HIV transmission is reduced by an estimated 95% for those on therapy.
First-line treatment regimens include two nucleotide/nucleoside reverse transcriptase inhibitors (abacavir/lamivudine or tenofovir/emtracitabine) with either an integrase inhibitor (eg dolutegravir, elvitegravir, or raltegravir), a non-nucleoside reverse transcriptase inhibitor (eg efavirenz), or a ritonavir-boosted protease inhibitor (eg darunavir, atazanavir).
Further reading: JAMA 2014; 312:410
Pharmacotherapy with what other agent would likely reduce the mortality risk in this patient?
Answer
[/accordion_item]
[accordion_item title=”CASE 7 – 37 year old with hepatitis B”]
A 37 year old gentleman, originally from Tanzania, presents for his annual health promotion visit. On routine laboratory screening, he is found to test positive for hepatitis B surface antigen. Further testing shows: HBeAg negative, HBeAb positive, HIV seronegative, HCV non-infected, HAV IgG positive, HBV DNA 1,700 IU/mL, platelets of 259 thousand/mL, AST 37 U/L, ALT 42 U/L and normal renal function. He feels well, has no signs of cirrhosis on physical exam, and was unaware of his hepatitis B infection.
aldosterone receptor antagonist (eg spironolactone, eplerenone)
Discussion: Aldosterone receptor antagonists are recommended in patients with NYHA class II-IV heart failure and who have an LVEF < 35%, to reduce morbidity & mortality. Creatinine in men should be < 2.5 mg/dL and in women < 2.0 mg/dL, and potassium < 5.0 mEq/L. Renal function and electrolytes should be carefully monitored after initiation. The landmark RALES study showed a 30% reduction in mortality and 35% reduction in hospitalizations during the 2-year follow-up of 1600+ patients.
For spironolactone, start at 12.5 – 25 mg per day; or for those with eGFR 30-49 ml/min/1.73 m2, it is appropriate to use every other day dosing. Monitor electrolytes and renal function after 2-3 days, then again at 7 days after initiation. Thereafter, monitoring should be done based on stability of renal function, and every 3 months if stable.
Further reading: NEJM 1999; 341:709
Discussion: Aldosterone receptor antagonists are recommended in patients with NYHA class II-IV heart failure and who have an LVEF < 35%, to reduce morbidity & mortality. Creatinine in men should be < 2.5 mg/dL and in women < 2.0 mg/dL, and potassium < 5.0 mEq/L. Renal function and electrolytes should be carefully monitored after initiation. The landmark RALES study showed a 30% reduction in mortality and 35% reduction in hospitalizations during the 2-year follow-up of 1600+ patients.
For spironolactone, start at 12.5 – 25 mg per day; or for those with eGFR 30-49 ml/min/1.73 m2, it is appropriate to use every other day dosing. Monitor electrolytes and renal function after 2-3 days, then again at 7 days after initiation. Thereafter, monitoring should be done based on stability of renal function, and every 3 months if stable.
Further reading: NEJM 1999; 341:709
Does this patient require treatment with antivirals? Does this patient require an ultrasound for hepatocellular carcinoma screening?
Answer
[/accordion_item]
[accordion_item title=”CASE 8 – 68 year old woman presenting for pre-operative cardiovascular risk assessment”]
A 68 year old woman with a history of intermittent symptoms consistent with biliary colic presents to clinic for discussion of peri-operative cardiovascular risks associated with a cholecystectomy. Surgery would be attempted as laparoscopic with possible need for open conversion. She has a history of coronary artery disease, s/p drug-eluting stent 6 years prior for a STEMI, and has not had anginal symptoms or dyspnea since. A TTE one year prior showed an LVEF of 55%, and she has no symptoms of heart failure. She has type II diabetes, well controlled on glargine, lispro and metformin. Her hypertension is well controlled on lisinopril. Her diabetes labs showed a HbA1c of 7.1% and creatinine of 0.8 mg/dL. She lives independently. She is a never-smoker. Her height is 5’4″, weight is 180 lbs.
No, antivirals are not needed at this time. Yes, HCC screening is indicated.
Discussion: This patient’s HBeAg is negative. The HBeAg is a marker of increased viral replication. Being negative, we expect the HBV DNA viral load to be low, as it is. For HBeAg-negative cases, the DNA threshold of increased concern is 2,000 IU/mL. With normal transaminases – suggesting little to no active hepatic inflammation – follow-up with monitoring is the recommended management plan. Follow-up with transaminases every 3 months initially, with recheck of HBV DNA and the HBeAg periodically (likely q 6 months initially or if transaminases are elevated). Antivirals are not indicated at this time.
He does merit screening for hepatocellular carcinoma, ideally with ultrasound, every 6-12 months. The 2009 AASLD guidelines for HCC screening are based on risk and recommend screening all African patients with HBV who are over 20 years of age (the presumption is that infection likely occurred at birth, and that these patients have had HBV for their entire life). See the guidelines for other populations for which HCC screening is recommended.
Further reading: Lok, Hepatology 2009; 50:661
Discussion: This patient’s HBeAg is negative. The HBeAg is a marker of increased viral replication. Being negative, we expect the HBV DNA viral load to be low, as it is. For HBeAg-negative cases, the DNA threshold of increased concern is 2,000 IU/mL. With normal transaminases – suggesting little to no active hepatic inflammation – follow-up with monitoring is the recommended management plan. Follow-up with transaminases every 3 months initially, with recheck of HBV DNA and the HBeAg periodically (likely q 6 months initially or if transaminases are elevated). Antivirals are not indicated at this time.
He does merit screening for hepatocellular carcinoma, ideally with ultrasound, every 6-12 months. The 2009 AASLD guidelines for HCC screening are based on risk and recommend screening all African patients with HBV who are over 20 years of age (the presumption is that infection likely occurred at birth, and that these patients have had HBV for their entire life). See the guidelines for other populations for which HCC screening is recommended.
Further reading: Lok, Hepatology 2009; 50:661
In her case, what is her risk class according to the Revised Cardiac Risk Index for pre-operative risk? And according to the American College of Surgeons Surgical Risk Calculator?
Answer
[/accordion_item]
[accordion_item title=”CASE 9 – 69 year old with back pain”]
A 69 year old gentleman presents again to primary care for continued lumbar back pain. His pain has been ongoing for 6 months, worsening per his report. His pain started gradually, is localized to the lumbar region, is not improved or relieved with position, does not radiate, is always present but varies in intensity, worsening after significant activity. He denies any neurologic symptoms. He gets no relief from acetaminophen, only modest relief from NSAIDs. He has a history of hypertension, hyperlipidemia, and gout. He denies any prior surgeries. He is a never-smoker, denies any alcohol use or IVDU and has a stable living situation. He has no family history of cancers. He take HCTZ, atorvastatin, allopurinol and aspirin. Physician exam is unremarkable. Recently laboratory work showed normal sodium, potassium, calcium; normal BUN and creatinine; AST 23 units/L, ALT 17 units/L, alk phos 170 IU/L, albumin 3.9; Hct 39%, WBC 5.4 thousand, normal platelet count.
Per the RCRI: Class III vs IV, 6.6 vs 11% risk (see below). Per the American College of Surgeons Surgical Risk Calculator: 3.4 – 4.6% risk of any complication, 2.7% risk of severe complication.
Discussion: The purpose of estimating the risk of a major adverse cardiac event (MACE) in the peri-operative period for a non-emergent, non-cardiac surgery is to help decide whether diagnostics to uncover occult or worsening cardiopulmonary disease (with purpose of then addressing & optimizing these underlying conditions) would result in better long-term outcomes for the patient, and ultimately avoid MACEs. Given fluid shifts and additional physiologic stressors during the peri-operative period, the risk for MACEs is increased as compared to usual activity.
The revised cardiac risk index is a validated tool for estimated risk, based on six risk factors: creatinine > 2 mg/dL, heart failure, insulin-dependent diabetes, history of a CVA or TIA, known ischemic heart disease, or that the planned surgery is high risk (intraperitoneal, intrathoracic, or suprainguinal vascular surgery). Class I (zero factors) estimates 0.4%; class II (1 factor) 0.9%; class III (2 factors) 6.6%, class IV (>2 factors) 11% or higher. The RCRI did not distinguish between laparoscopic and open intraperitoneal surgeries, a limitation in its use. Thus, our patient may be considered to have 2 or 3 risk factors, depending on whether laparoscopic cholecystectomy is considered high-risk.
The American College of Surgeons Surgical Risk calculator (http://riskcalculator.facs.org) uses an increased number of factors to estimate risk. This has not been validated outside the original population from which it was derived. Another limitation is the inclusion of the ill-defined American Society of Anesthesiology Physical Status Classification. Our patient may be assumed to have a physical status of class II or III, resulting the risks as noted above.
If this patient were unable to meet 4 METs of physical activity, then based on the risks above, further cardiac testing would be merited.
Further reading: PMID: 25091544; and Lee, Circulation 1999; 100:1043
Discussion: The purpose of estimating the risk of a major adverse cardiac event (MACE) in the peri-operative period for a non-emergent, non-cardiac surgery is to help decide whether diagnostics to uncover occult or worsening cardiopulmonary disease (with purpose of then addressing & optimizing these underlying conditions) would result in better long-term outcomes for the patient, and ultimately avoid MACEs. Given fluid shifts and additional physiologic stressors during the peri-operative period, the risk for MACEs is increased as compared to usual activity.
The revised cardiac risk index is a validated tool for estimated risk, based on six risk factors: creatinine > 2 mg/dL, heart failure, insulin-dependent diabetes, history of a CVA or TIA, known ischemic heart disease, or that the planned surgery is high risk (intraperitoneal, intrathoracic, or suprainguinal vascular surgery). Class I (zero factors) estimates 0.4%; class II (1 factor) 0.9%; class III (2 factors) 6.6%, class IV (>2 factors) 11% or higher. The RCRI did not distinguish between laparoscopic and open intraperitoneal surgeries, a limitation in its use. Thus, our patient may be considered to have 2 or 3 risk factors, depending on whether laparoscopic cholecystectomy is considered high-risk.
The American College of Surgeons Surgical Risk calculator (http://riskcalculator.facs.org) uses an increased number of factors to estimate risk. This has not been validated outside the original population from which it was derived. Another limitation is the inclusion of the ill-defined American Society of Anesthesiology Physical Status Classification. Our patient may be assumed to have a physical status of class II or III, resulting the risks as noted above.
If this patient were unable to meet 4 METs of physical activity, then based on the risks above, further cardiac testing would be merited.
Further reading: PMID: 25091544; and Lee, Circulation 1999; 100:1043
Given the duration and worsening pain, radiographs were obtained, with area of interested highlighted here:

What is the likely diagnosis? What are your next steps in work-up or management?
Answer
[/accordion_item]
[accordion_item title=”CASE 10 – 43 year old with nephrolithiasis”]
A 43 year old gentleman presents for post-emergency room follow-up. He was seen in the ER 7 days prior for left flank pain, diagnosed with symptomatic nephrolithiasis. He passed the stone in the emergency room. The stone was sent for analysis, returning as a calcium oxalate stone. He currently feels well, without complaints. He has no other past medical or surgical history. He takes no medications.
Paget’s disease of bone
Discussion: Paget’s affects predominantly those of European descent, with prevalence rates of 5% of women and 8% of men by their 70s. The most common symptom is persistent bone pain, often in the pelvis, femur, lumbar spine, skull or tibia.
Paget’s is an as-yet idiopathic process of increased and disorganized bone remodeling in focal areas throughout the skeleton. Many cases, however, never come to medical attention. Complications can include spinal stenosis, increased osteoarthritis, and high-output cardiac failure (due to arteriovenous shunts within affected bone).
Radiographs show a typical appearance of enlarged bone, often with increased opacification (though this depends on the stage). In the spine, an “ivory vertebrae” can sometimes be seen, as above, with an appearance of coarsening of the trabecular pattern. The alkaline phosphate is typically (but not always) elevated, with other labs normal. Also on the differential is lymphoma and metastases, and several less common bone disorders. Laboratory work-up to look for other signs of disease (CMP, vitamin D, calcium level). The radiographic appearance often assists to arrive at a diagnosis or at least narrow the differential. A bone scan – for a baseline picture of which bones Paget’s is affecting – is often done. Treatment is with bisphosphonates.
Further reading: Ralston, NEJM 2013; 368: 644
Discussion: Paget’s affects predominantly those of European descent, with prevalence rates of 5% of women and 8% of men by their 70s. The most common symptom is persistent bone pain, often in the pelvis, femur, lumbar spine, skull or tibia.
Paget’s is an as-yet idiopathic process of increased and disorganized bone remodeling in focal areas throughout the skeleton. Many cases, however, never come to medical attention. Complications can include spinal stenosis, increased osteoarthritis, and high-output cardiac failure (due to arteriovenous shunts within affected bone).
Radiographs show a typical appearance of enlarged bone, often with increased opacification (though this depends on the stage). In the spine, an “ivory vertebrae” can sometimes be seen, as above, with an appearance of coarsening of the trabecular pattern. The alkaline phosphate is typically (but not always) elevated, with other labs normal. Also on the differential is lymphoma and metastases, and several less common bone disorders. Laboratory work-up to look for other signs of disease (CMP, vitamin D, calcium level). The radiographic appearance often assists to arrive at a diagnosis or at least narrow the differential. A bone scan – for a baseline picture of which bones Paget’s is affecting – is often done. Treatment is with bisphosphonates.
Further reading: Ralston, NEJM 2013; 368: 644
What would be your recommendations to reduce this gentleman’s risk of developing future kidney stones?
Answer
[/accordion_item]
[accordion_item title=”CASE 11 – 40 year old woman inquiring about mammography”]
A 40 year old woman, with no family or personal history of breast or ovarian cancer, asks her primary care provider if she needs a mammogram. She has never received a mammogram, and, based on self-breast exam, has no immediate concerns. She is asymptomatic.
Increase fluid intake to maintain urine output > 2 liters/day; diet high in calcium and low in sodium; possible thiazide diuretic for recurrent stones. Other interventions based on 24-hour urine results (if obtained, see below)
Discussion: 80% of kidney stones are calcium oxalate (often with variable calcium phosphate mixed in). Diagnosis of the type of stone requires collection of the stone and sending to the lab for analysis. After a first kidney stone, the need for extensive work-up is debatable. Stone analysis and checking a BMP are generally recommended to identify the type of stone and to screen for chronic kidney disease, hypercalcemia (which if found, would prompt further work-up) and suggestions of renal tubular acidosis (based on HCO3-). High intake of low-solute/low-sodium fluid to produce urine output > 2 liters/day and a diet high in calcium are recommendations applicable to all with calcium-based stones. High urine output dilutes the calcium and oxalate (or phosphate) in the urine, reducing concentrations and the probability of crystallization. High calcium diet increases the amount of calcium in the gut, which binds to oxalate in the gut, effectively preventing the absorption of oxalate and reducing kidney stone recurrences.
For recurrent stones, obtain a 24-hour urine for measurement of urine calcium, oxalate, uric acid, citrate and creatinine. Urine creatinine assesses the accuracy of the measurement (as estimates can be made based on urine creatinine if the sample appears consistent with a 24-hour urine collection). Patients with hypercalciuria especially benefit from low sodium and low animal protein diets and from thiazide diuretics – all serving to reduce the calcium concentration in the distal tubules. Other interventions: low oxalate diets for hyperoxaluria; potassium citrate supplements for hypocitraturia (K-citrate helps bind to calcium); and allopurinol for hyperuricosuria (uric acid decreases calcium solubility).
Further reading: Worcester, NEJM 2010; 363:954
Discussion: 80% of kidney stones are calcium oxalate (often with variable calcium phosphate mixed in). Diagnosis of the type of stone requires collection of the stone and sending to the lab for analysis. After a first kidney stone, the need for extensive work-up is debatable. Stone analysis and checking a BMP are generally recommended to identify the type of stone and to screen for chronic kidney disease, hypercalcemia (which if found, would prompt further work-up) and suggestions of renal tubular acidosis (based on HCO3-). High intake of low-solute/low-sodium fluid to produce urine output > 2 liters/day and a diet high in calcium are recommendations applicable to all with calcium-based stones. High urine output dilutes the calcium and oxalate (or phosphate) in the urine, reducing concentrations and the probability of crystallization. High calcium diet increases the amount of calcium in the gut, which binds to oxalate in the gut, effectively preventing the absorption of oxalate and reducing kidney stone recurrences.
For recurrent stones, obtain a 24-hour urine for measurement of urine calcium, oxalate, uric acid, citrate and creatinine. Urine creatinine assesses the accuracy of the measurement (as estimates can be made based on urine creatinine if the sample appears consistent with a 24-hour urine collection). Patients with hypercalciuria especially benefit from low sodium and low animal protein diets and from thiazide diuretics – all serving to reduce the calcium concentration in the distal tubules. Other interventions: low oxalate diets for hyperoxaluria; potassium citrate supplements for hypocitraturia (K-citrate helps bind to calcium); and allopurinol for hyperuricosuria (uric acid decreases calcium solubility).
Further reading: Worcester, NEJM 2010; 363:954
When would you recommend starting screening mammograms? At what interval would you recommend they continue?
Bonus: For 1000 women at age 50, undergoing annual mammography for 10 years, how many deaths due to breast cancer would you estimate would be prevented? How many would be estimated to be overdiagnosed and treated, unnecessarily, with surgery, radiation or chemotherapy?
it’s complicated
Bonus Answer: 0.3 – 3.2 breast cancer deaths avoided. 3-14 women would be overdiagnosed and treated unnecessarily
Discussion:
While this may be surprising to some, mammography is actually quite controversial. Recommendations & opinions on routine screening mammography range from starting at age 40, annually, to not doing any screening at all. The USPSTF recommends starting at age 50, with q 2 year mammography until age 74.
The data supporting mammography is modest at best. The recently released 25-year follow-up data from the Canadian National Breast Screening study (Miller 2014), which randomized women ages 40-59 to annual mammography x 5 years or routine care (no mammography at the time), showed no reduction in breast cancer mortality, but did show a 22% increase in over-diagnosis and treatment. A 2013 Cochrane review showed that, among 3 trial with adequate randomization, there was no reduction in breast cancer mortality, total cancer mortality or all-cause mortality. When 4 trials with suboptimal randomization were included, there was a 19% decrease in breast cancer mortality. The Welch 2014 article summarize the risks and benefits of screening mammography based on age group.
The decision to screen includes consideration of multiple factors: the risk of overdiagnosis, the risk of false positives, the individual risk of the patient, and the patient values. See the below articles for succinct summaries of the controversy & data.
Further reading:
Welch, JAMA Intern Med 2014; 174:448.
Gøtzsche, Cochrane Database of Systematic Reviews 2013; 6:CD001877
Biller-Andorno, NEJM 2014; 370:21
Bonus Answer: 0.3 – 3.2 breast cancer deaths avoided. 3-14 women would be overdiagnosed and treated unnecessarily
Discussion:
While this may be surprising to some, mammography is actually quite controversial. Recommendations & opinions on routine screening mammography range from starting at age 40, annually, to not doing any screening at all. The USPSTF recommends starting at age 50, with q 2 year mammography until age 74.
The data supporting mammography is modest at best. The recently released 25-year follow-up data from the Canadian National Breast Screening study (Miller 2014), which randomized women ages 40-59 to annual mammography x 5 years or routine care (no mammography at the time), showed no reduction in breast cancer mortality, but did show a 22% increase in over-diagnosis and treatment. A 2013 Cochrane review showed that, among 3 trial with adequate randomization, there was no reduction in breast cancer mortality, total cancer mortality or all-cause mortality. When 4 trials with suboptimal randomization were included, there was a 19% decrease in breast cancer mortality. The Welch 2014 article summarize the risks and benefits of screening mammography based on age group.
The decision to screen includes consideration of multiple factors: the risk of overdiagnosis, the risk of false positives, the individual risk of the patient, and the patient values. See the below articles for succinct summaries of the controversy & data.
Further reading:
Welch, JAMA Intern Med 2014; 174:448.
Gøtzsche, Cochrane Database of Systematic Reviews 2013; 6:CD001877
Biller-Andorno, NEJM 2014; 370:21
If he had little pain to tugging on the tragus and pinna, with an otoscopic exam as below, what might be your management?
If he had more significant pain and an otoscopic exam as below, what might be your management?
[/accordion_item]